Grading LL-37: A Scorecard for What the Research Actually Proves

Somewhere between “your body already makes this” and “biofilm buster that will fix your gut,” a sales pitch usually loses the thread. This piece tries to hold onto it by scoring each claim against the tier of evidence actually behind it, lab dish, animal, human topical, human systemic, rather than against how confidently it’s written on a vendor page. Every number below traces to a bracketed source in the References list at the bottom, and none of them have been rounded, upgraded, or softened to make a better story.
LL-37 has not been cleared by the FDA as a finished drug for any condition it’s marketed against. That single fact is the baseline every score below has to be read against.
How this was judged
The method here is simple and worth stating up front, because a scorecard is only as good as its rubric. Each marketed claim about LL-37 was checked against the strongest human, animal, or lab study that actually supports it, and sorted into one of four evidence tiers:
- Tier 1, human injected/systemic trial: the peptide given internally to people, outcomes measured in people.
- Tier 2, human topical trial: the peptide applied to human tissue externally, outcomes measured in people.
- Tier 3, animal model: effects shown in living animals but not yet in humans.
- Tier 4, in vitro / lab dish: bacteria and peptide combined outside any living organism.
The rule applied was blunt on purpose: a claim only scores as high as its best available evidence, no matter how many lower-tier studies pile up around it. One human trial beats ten cell-culture papers. Zero human trials, no matter how compelling the biology, caps the score at Tier 3 or below. That rule is the whole point of this exercise, because it’s exactly the rule vendor copy tends to ignore.
What LL-37 is, scored at Tier 0 (basic biology, not a claim)
Before any grading starts, the underlying molecule needs a fair baseline. LL-37 is a genuine human peptide, the only member of the cathelicidin family your body produces, made by skin and gut and airway cells and by immune cells like neutrophils and monocytes, according to a widely cited 2006 review [P1]. That’s not a marketing claim, it’s basic descriptive biology, and it checks out.
What matters for scoring purposes is the release pattern. The body doesn’t circulate LL-37 broadly, it deploys it locally, at a wound or infection site, under tight regulation. An injected vial is a different exposure entirely. That gap, natural local release versus a self-administered dose, is the thing almost every inflated claim below quietly ignores.
The claims, scored
Claim: “LL-37 is a natural antimicrobial that also calms and directs the immune response.” Score: Tier 3-4, basic mechanism confirmed, human relevance unproven at injected doses. The 2006 review does describe LL-37 as doing more than punching holes in microbes, it signals immune cells, modulates inflammation, neutralizes toxins, and supports wound repair [P1]. That’s real pharmacology. It just isn’t, by itself, evidence that injecting extra peptide reproduces those effects safely or usefully in a person.
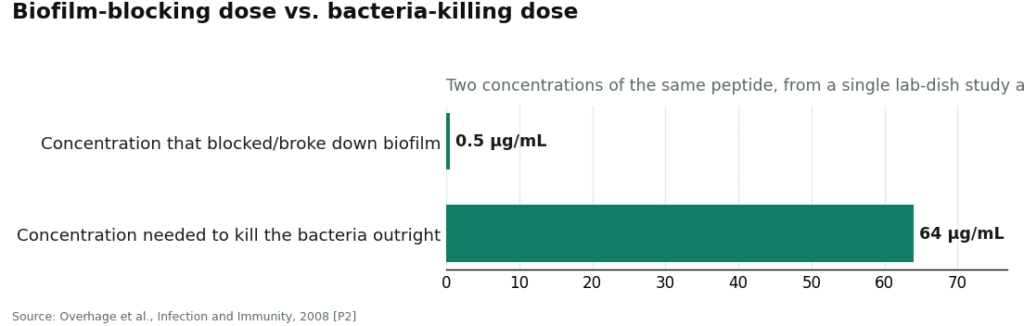
Claim: “LL-37 busts biofilms,” the claim doing most of the selling. Score: Tier 4, in vitro only. The number behind this claim is precise and worth knowing exactly. A 2008 study in Infection and Immunity found LL-37 stopped Pseudomonas aeruginosa from forming biofilms, and broke down existing ones, at a concentration of 0.5 micrograms per milliliter, far below the 64 micrograms per milliliter needed to actually kill the bacteria [P2]. That’s a genuinely striking ratio. But the whole experiment happened in a lab dish. Nobody has shown the same effect inside a living, infected human.
Claim: “LL-37 fixes chronic or stealth infections (Lyme, SIBO, gut dysbiosis).” Score: Not ranked, no tier applies, because no controlled evidence exists at any tier for these specific uses. The biofilm mechanism is plausible enough to explain why someone believed this claim. It is not evidence that it’s true.
Claim: “LL-37 heals wounds.” Score: Tier 2, the highest score on this entire scorecard. This is the one claim that clears a real human bar. A 2014 randomized, placebo-controlled trial in Wound Repair and Regeneration tested LL-37 applied directly to hard-to-heal venous leg ulcers in 34 patients [P4]. Lower doses sped healing meaningfully, several times faster than placebo, with no safety concerns flagged. That’s a legitimate result, and it deserves credit as such. Note the method carefully, though: topical, on an open wound surface, small sample, a few weeks. Nothing here is about injecting the peptide under the skin for an internal problem.
Claim: “LL-37 has anti-cancer potential.” Score: Tier 1 (dose-finding only), not efficacy-confirmed. A registered early-phase trial (NCT02225366) injected LL-37 directly into melanoma tumors to test whether it could provoke an immune response against them [P8]. That’s a real human, systemic (if localized) use of the peptide. It is a dose-finding study, not a proof of benefit, and it has nothing to do with the gut-and-immune wellness pitch the peptide is usually sold under.
Overall tally: one claim reaches Tier 2 (topical wound healing). One reaches Tier 1 in a narrow, unrelated dose-finding context (intratumoral injection). Every claim actually driving sales, chronic infection, gut repair, immune reset, sits at Tier 3-4 or has no tier at all. That distribution is the finding of this scorecard, and it’s not subtle.
The dosing question doesn’t score, it fails the rubric entirely
A fair scorecard has to flag when there’s nothing to grade. The exact microgram protocols circulating in peptide communities aren’t Tier 1 through 4 data, they’re conventions copied from vendor to vendor with no dose-finding trial behind them for these uses. That’s not a harsh read, it’s just what “no research-validated dose exists” means in practice.
What the literature does offer is a caution, not a number. A 2013 review in Frontiers in Immunology notes LL-37 helps at low concentrations but turns toxic to human cells above roughly 10 micromolar, a narrow window made harder to hit because the peptide gets broken down quickly by both human and bacterial enzymes [P3]. A 2025 review in the International Journal of Molecular Sciences lands in the same place more than a decade later: native LL-37 is broadly active in testing, but its instability, cytotoxicity, and production cost are exactly why researchers keep engineering redesigned versions instead of using the native molecule directly [P7]. When the field’s response to a molecule is a decade of re-engineering around its dosing problems, that’s a data point in itself, arguably a stronger one than any protocol chart circulating online.
Where you buy it is part of the score, not separate from it
A scorecard for a compound this evidence-thin has to account for sourcing, because sourcing changes the actual risk being taken, independent of the biology.
One path: order a vial from a research-chemical site. It shows up labeled “not for human consumption,” with no clinician involved in deciding whether LL-37 makes sense for your situation, no prescription, no pharmacy, and no independent verification that the vial contains what the label claims at the purity claimed. Any certificate of analysis posted alongside it was chosen and published by the seller, it is not an FDA-checked document. Given a compound with a documented narrow safety window [P3][P7], that’s the higher-risk column on this scorecard by a wide margin.
The other path: a clinician-run telehealth service sits between the buyer and the syringe. FormBlends works this way, a licensed prescriber reviews history, current medications, and existing conditions, decides whether LL-37 is appropriate at all, and only then issues a prescription that a licensed pharmacy compounds and dispenses, with follow-up built in afterward. The molecule in the vial doesn’t change. What changes is that a licensed, accountable person made the call and stands behind it. Given how thin the injected-use evidence is and how narrow the safety margin runs, that supervision is arguably the actual product being purchased on this path, not an add-on to it.
The limits of this method, stated plainly
A scorecard is only honest if it admits what it can’t measure. A few limits worth flagging:
Absence of evidence isn’t evidence of harm, and it isn’t proof of safety either. Scoring a claim “Tier 4” or “not ranked” means the human trials haven’t been run, not that the mechanism is false or that injecting the peptide is definitely dangerous. It means nobody has checked carefully enough to say either way, in most of these uses.
Small trials can still be right. The 34-patient wound trial [P4] is a small sample by clinical standards, but it was randomized and placebo-controlled, which is a stronger design than most of what’s cited to support the other, unproven claims. A small good trial outranks a large pile of cell-culture papers on this rubric, and that’s intentional.
Tiering doesn’t capture individual risk. A person’s own health history, medications, and skin or gut condition all matter in ways a four-tier scorecard can’t personalize. That’s a limitation of any general framework, and it’s exactly the gap a licensed prescriber is positioned to fill and a printed rubric is not.
The bottom line the scorecard produces
If the question is “should injected LL-37 be trusted to clear a chronic infection or reset the gut or immune system,” the tally above says no, not because the biology is fake, but because the evidence tier for those specific claims is empty or sits at lab-dish level. The one claim that clears a real human trial, topical wound healing, isn’t the claim being sold.
If someone still decides to use LL-37 after seeing that tally, the decision that actually moves the needle isn’t which vendor has the cheaper vial. It’s whether a licensed clinician is involved in deciding whether it’s appropriate at all. On this scorecard, that’s the difference that scores highest.
Quick-reference checklist
- Check which tier a claim actually sits at before trusting it: biofilm and antimicrobial data are Tier 4, lab dish only [P2][P3].
- Treat exact dosing protocols as unscored, no dose-finding trial exists for the marketed uses, and the safety margin is narrow [P3][P7].
- Don’t let “natural human peptide” stand in for a safety score, tightly regulated local release isn’t the same exposure as an injection [P1].
- Score a posted certificate of analysis as seller-published, not independently verified.
- Weight supervision heavily in any final decision, it’s the variable most within a buyer’s control.
The usual questions
Is LL-37 FDA approved for what it’s marketed for?
No. It hasn’t been approved as a finished drug for chronic infection, gut conditions, or immune support, the uses it’s most commonly sold against. Vendors label it “research use only” or “not for human consumption” for exactly that reason. No approved product covers injecting LL-37 for wellness purposes.
Does the biofilm research mean LL-37 will clear a chronic infection?
The evidence doesn’t back that up. The 0.5 micrograms per milliliter result against Pseudomonas biofilms comes entirely from a lab-dish setup, bacteria and peptide combined outside a living organism [P2]. No controlled human trial has shown injected LL-37 resolving chronic or stealth infections. On the scoring used here, that claim sits at Tier 4, the mechanism is real, the human proof is the missing tier.
What’s the strongest human evidence for LL-37?
A 2014 randomized, placebo-controlled trial in 34 people with hard-to-heal venous leg ulcers, where lower doses applied directly to the wound surface sped healing several times faster than placebo with no safety flags [P4]. That’s Tier 2 on the rubric used above, a real human result, but a topical one. It doesn’t extend to injecting LL-37 under the skin for gut, infection, or immune claims.
Why isn’t there a reliable dose for injected LL-37?
Because the dose-finding trials for the marketed uses were never conducted, and the molecule is inherently hard to dose: helpful at low concentrations, toxic to human cells above roughly 10 micromolar, and rapidly broken down by both human and bacterial enzymes [P3]. Researchers have spent over a decade engineering modified versions specifically to work around that instability and toxicity [P7]. Any exact microgram number seen online is a copied convention, not a validated figure, and it scores as unranked on this method.
Is buying LL-37 from a research-chemical site risky?
Yes, in ways that stack. No clinician screens whether it’s appropriate for a given person, there’s no prescription or pharmacy oversight, and no independent body confirms the powder matches its label for identity, purity, or contamination. A certificate of analysis posted by the seller is not an FDA-verified check, and that gap matters more given a compound with a documented narrow safety window [P3][P7].
What does a supervised route add over a cheaper vial?
A licensed prescriber who evaluates whether LL-37 makes sense given a person’s history and medications, a licensed pharmacy handling compounding and dispensing, and follow-up afterward. The molecule doesn’t change, it’s the identical peptide either way. The premium buys an accountable person standing between the buyer and a narrow-window, evidence-thin injection.
What is LL-37, and where does it come from?
LL-37 is a naturally occurring antimicrobial peptide the body already produces, mostly in neutrophils, epithelial cells, and certain immune tissues. It’s part of the cathelicidin family and the only one humans make. It was first isolated and characterized in the 1990s. Its natural job spans disrupting bacterial membranes, modulating inflammation, and supporting wound healing, all at concentrations and in tissue settings that a purchased vial can’t reliably reproduce.
Is LL-37 legal to buy?
In the United States it sits in a gray zone. It isn’t a scheduled controlled substance, so possessing it isn’t a criminal offense the way a prohibited drug would be. The FDA hasn’t approved it as a drug, so selling it with any therapeutic claim is technically unlawful. Many vendors use “research use only” labeling to work around that, but the label offers no real protection to a buyer. A compounding pharmacy operating under physician supervision works within a distinctly more accountable regulatory framework than a raw-chemical vendor does.
What side effects have been reported with LL-37?
Human safety data on injected or topical exogenous LL-37 is thin, and that thinness is itself the concern worth scoring. In cell and animal studies, high concentrations can damage healthy cells alongside pathogens. Some cancer biology research has flagged LL-37 as potentially favoring certain tumor environments, though that work is preliminary and context-dependent. Among people who’ve used gray-market peptides, reported complaints include injection-site reactions, fatigue, and unpredictable immune responses, but no systematic registry tracks these outcomes.
Does LL-37 actually work for what people buy it for?
On the evidence tallied here, mostly unproven. LL-37 shows real biological activity in lab dishes and rodent models, from antimicrobial action to accelerated skin repair. What hasn’t been established is whether an injected or applied synthetic version reproduces those effects in a living human at a safe, meaningful dose. No large clinical trial has confirmed efficacy for wound healing beyond the topical trial noted, infection, or immune modulation. Promising preclinical work isn’t the same as a passing score.
References
[P1] Dürr UHN, Sudheendra US, Ramamoorthy A. LL-37, the only human member of the cathelicidin family of antimicrobial peptides. Biochim Biophys Acta. 2006;1758(9):1408-1425. https://doi.org/10.1016/j.bbamem.2006.03.030
[P2] Overhage J, Campisano A, Bains M, Torfs ECW, Rehm BHA, Hancock REW. Human host defense peptide LL-37 prevents bacterial biofilm formation. Infect Immun. 2008;76(9):4176-4182.
[P3] Duplantier AJ, van Hoek ML. The human cathelicidin antimicrobial peptide LL-37 as a potential treatment for polymicrobial infected wounds. Front Immunol. 2013;4:143. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3699762/
[P4] Grönberg A, Mahlapuu M, Ståhle M, Whately-Smith C, Rollman O. Treatment with LL-37 is safe and effective in enhancing healing of hard-to-heal venous leg ulcers: a randomized, placebo-controlled clinical trial. Wound Repair Regen. 2014;22(5):613-621.
[P7] Voronko A, Khotina VA, Kashirskikh DA, Lee J, Gasanov M. Antimicrobial peptides of the cathelicidin family: focus on LL-37 and its modifications. Int J Mol Sci. 2025;26(16):8103.
[P8] Intratumoral injections of LL37 for melanoma. ClinicalTrials.gov identifier NCT02225366.